Hip Dysplasia Specialist

Do you have frequent hip dislocations, hip pain or the feeling that your hip will not stay in the joint? You may have been diagnosed with hip dysplasia or you may have developed hip dysplasia. Hip dysplasia is common in families, and especially in females. Adolescents with hip dysplasia need to seek early treatment. Doctor Benedict Nwachukwu provides diagnosis as well as surgical and nonsurgical treatment options for patients in Manhattan, Brooklyn, and New York City, NY who are experiencing complications from hip dysplasia. Contact Dr. Nwachukwu’s team today!
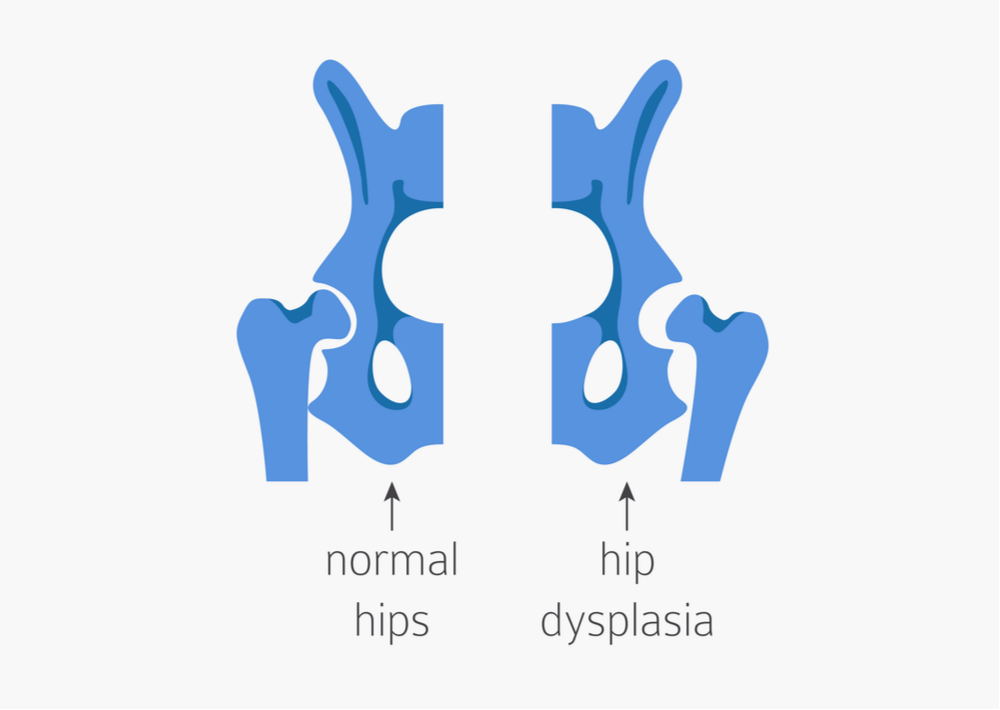
What is hip dysplasia?
The hip is a ball and socket joint that when functioning properly, the ball of the femoral head (thigh bone) is held securely within the socket of the acetabulum (hip bone). Hip dysplasia occurs when the hip socket does not fully cover the ball portion of the thigh bone. Hip dysplasia can cause hip instability, recurrent dislocations, joint pain and eventually osteoarthritis. Most people who have hip dysplasia are born with this condition. Dr. Benedict Nwachukwu, orthopedic hip specialist serving Manhattan, Brooklyn, New York City and surrounding New York boroughs is highly trained and experienced at diagnosing and treating hip dysplasia.
What are the classifications of hip dysplasia?
Hip dysplasia is often characterized by when it occurs in a patient’s life, as well as the severity of the symptoms. The classifications for hip dysplasia can include:
- Developmental Dysplasia of the Hip (DDH) – Is the preferred term for babies and children that develop hip dysplasia.
- Congenital Dislocation of the Hip (CDH) – Refers to the malformation of the hip joint during fetal development.
- Acetabular Dysplasia – Occurs when there is inadequate development of an individual’s acetabulum during the adolescent and teenage years.
What are the types of hip dysplasia?
In addition to the specific classifications of hip dysplasia, there are terms describing how the head of the femur is held into the acetabulum or socket of the hip. These terms include:
- Acetabular Dysplasia: The ball of the femur remains in the socket of the hip, but the socket is too shallow to keep the ball firmly in place.
- Subluxable: The ball of the femur is in its correct position in the socket of the hip, however pushing on the hip or changing positions can move the ball partially out of the socket.
- Subluxed: Occurs when the ball of the femur is not within the socket, but rests partway out.
- Dislocatable: When the ball of the hip is easily dislocated out of the socket.
- Dislocated: The hip is completely out of the socket. Different from subluxed, the ball no longer rests near the socket but is completely removed from the socket.
What causes hip dysplasia?
There are risk factors that predispose adolescents to hip dysplasia. These risk factors can be:
- Heredity: Often Developmental Dysplasia of the Hip (DDH) runs in families and is an inherited trait.
- Gender: Females are 4 to 5 times more likely to have hip dysplasia than males.
- Breech birth: When a baby is born bottom first.
- Firstborn: More commonly, first-born children have hip dysplasia than subsequent siblings.
- Twins or multiple gestations: Twins, triplets, etc. have a higher risk for hip dysplasia. If for instance, one twin is born with DDH the other twin is 40% more likely to also have DDH.
What are the symptoms of hip dysplasia?
The symptoms of hip dysplasia can vary depending on age but in adults and adolescents the symptoms can include:
- Pain in the side of the hip
- Pain in the groin area
- Limping
- Popping or catching sensation with activity
- Difficulty with strenuous activities
- A feeling of the hip giving way
- Early arthritis
How is hip dysplasia diagnosed?
Physicians typically check for hip dysplasia in infants by gently moving the legs in different positions. In patients who develop the condition later in life, a physical examination, medical history review and an x-ray evaluation need to be performed by Dr. Nwachukwu to diagnose the condition. He may also request an MRI to make an accurate diagnosis and to determine if soft tissues, such as the labrum have been damaged or are involved in hip dysplasia.
How is hip dysplasia treated?
Non-Surgical
In patients with mild dysplasia and limited pain symptoms, non-operative treatment can be considered. Non-operative treatment options include:
- Weight loss
- Lifestyle Modification
- Joint injections
- Specialized physical therapy
- Cycling or swimming instead of high impact sports, like running or basketball which puts added stress on the joint
In patients with moderate to severe dysplasia and hip pain there is consensus that non-operative treatment is not preferred due to an increased risk for progression to hip osteoarthritis.
Surgical
Adolescents and adults often require surgery to alleviate the symptoms of hip dysplasia. Depending on the severity and symptoms of the dysplasia as well as the goals of the patient, Dr. Nwachukwu may recommend one of the following:
- Periacetabular Osteotomy (PAO): When the bone is cut around the hip socket and repositioned so it can fit better within the hip socket.
- Arthroscopic Hip Surgery: (Please read Dr. Nwachukwu’s study about treating Hip Dysplasia with Arthroscopic FAI Surgery HERE) In patients with borderline hip dysplasia, hip arthroscopy is a good treatment option to address problems related to hip impingement. Hip dysplasia leads to excessive hip motion thereby creating a type of dynamic hip impingement that can cause tearing of the hip labrum. Hip arthroscopy for mild dysplasia involves surgery to fix the hip labrum and tightening of the hip joint capsule.
- Hip Arthroplasty or Joint Replacement Surgery: In most cases, the goal is to preserve the original hip and Dr. Nwachukwu usually considers joint replacement only in advanced cases of osteoarthritis.
How long is the recovery after hip dysplasia surgery?
Following any kind of arthroscopic or open hip surgery, it is essential that patients follow Dr. Nwachukwu’s post-op recovery protocol. This will give them the best possible chance for a full recovery. Typically, a well-supervised physical therapy program will help establish full range of motion and mobility. Dr. Nwachukwu’s patients begin with a highly skilled physical therapist immediately following surgery. For patients who have to travel for this specialized surgery, the same protocol will be provided to allow continued success once they are back home.
For more information and treatment options for hip dysplasia please contact the office of Benedict Nwachukwu, MD, orthopedic hip specialist serving Manhattan, Brooklyn, New York City and surrounding New York boroughs.